Location & Hours
4008 Red Cedar Dr D-1
Highlands Ranch, CO 80126-8152
| Mon & Fri: | 8 - 4 |
| Tues - Thurs: | 10 - 7 |

More middle-aged and older adults are wearing soft contacts than ever.
And one of the biggest reasons they stop wearing contacts is the difficulty they face reading with their contacts after presbyopia begins to set in around the early 40’s.
Presbyopia is the diminished ability of the natural lens in our eyes to focus up on close objects. It begins with the occasional medicine bottle being a struggle to read and then over time more and more gets blurry. It can be very frustrating to stare at something up close and have it be blurry regardless of what you do.
So there are three basic choices a contact lens wearer can do to aid their reading while still wearing contact lenses.
Reading Glasses
Initially, the use of an over-the-counter reader or prescription reading glass for occasional use works well for people in the early stages of presbyopia. They are worn over distance contact lenses so there is little adjustment and vision is clear near and far. However, they need to be with you, not left in the car or at work, and oftentimes people end up just wearing readers all day since it is just that much clearer.
Monovision
This fitting technique can be used with any type of contact lens. The brand of lenses you are currently wearing can often be used to fit you with monovision. Your dominant eye is determined. Then the non-dominant eye prescription is adjusted to compensate to make it a reading contact lens. So once fitted you have one eye for distance and the other for reading. Yes, it sounds really crazy, but it can actually work quite well. Your brain initially has to adjust to using each eye individually to obtain the sharpest vision, but once this is achieved, year-to-year adjustments can be made to the reading eye to allow comfortable distance and reading vision for many years.
Monovision fits are not always successful. Some people just cannot adjust to it regardless of motivation or desire. It seems to work best when someone has had some difficulty with reading and they are noticing more and more that they need their readers. At that point, they can appreciate the ability to read and their brain seems to adapt more readily. When I wear my contacts this is the option I have used for myself.
Multifocal Contacts
Another option is multifocal contact lenses. Most major manufacturers of soft contact lenses have some type of disposable multifocal lens available. They do not work like multifocal glasses. They use a technique called simultaneous viewing where you are actually looking through all the powers at once.
To visualize this, imagine a vinyl record with the label in the center and the various tracks extending outward. Most of the lenses are made with the strongest reading power located in the center where the label would be, then each ring further out gradually becomes weaker until you reach your full distance power. So essentially you are looking “around” the reading part for distance then through the center for reading. It works, sort of.
Multifocal lenses work better on younger patients, say 40-50 years old, for help with reading. There is no adaptation period to these lenses like monovision. What you see is what you get. But if you have any significant amount of astigmatism or if you wear a toric contact that corrects for astigmatism, multifocal lenses are not for you. And because the reading is central in the lens, if you make it too strong for reading then you blur the distance vision too much, so oftentimes a multifocal lens wearer after age 50 faces the dilemma of either wearing reading glasses to boost their reading needs or changing to monovision.
Conclusion
In conclusion, while none of the options are perfect, they all may present some level of relief in your quest to continue to wear contacts into middle age, retirement, and beyond. But some options may better serve you at a certain point in your life or career than others. Talk to your eye doctor to see what choices are best for you.
Article contributed by Eugene Schoener O.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Motherhood...the sheer sound of it brings enduring memories. A mother’s touch, her voice, her cooking, and the smile of approval in her eyes. Science has proven that there is a transference of emotion and programming from birth and infancy between a mother and her child--a type of communication, if you will, that occurs when the infant looks into its mother’s eyes. So what is this programming? How does it work and what effect does it have on the life of the child? What happens if it never happened to the infant? What happens if the mother is blind?
The gaze into a mother’s eyes brings security and well being to the child. When she gazes at another person, it makes the infant look at what she is gazing at, and introduces the infant to others in the world. This is known as a triadic exchange. So now the baby's world is no longer just one person--its mother--but also includes third parties, thereby increasing social skills and interaction.
Interestingly, if a mother is blind, it does not adversely affect the child’s development. A study published in the Proceedings of the Royal Society B showed no deficit in the baby's advancement. The sheer fact that the infant looks into the mother’s eyes helps with connectedness and emotional grounding.
Looking into mom’s eyes and face teaches facial recognition and expressions of emotions and is primarily how the child learns in the first few months of life. Additionally, infants tend to show a preference to viewing faces with open eyes rather than closed eyes, thus stressing the importance of the mother or caregiver’s gaze.
Some health benefits to gazing into the mother’s eyes is a lower incidence of autism, or spectrum disorders, and better social skills, higher learning capacity, and emotional groundedness.
The beauty of a mother’s gaze is that the child can feel the emotions of love, security, safety, and overall well-being by connecting with her through eye-to-eye contact. This sets the stage for the future development of social skills, visual recognition of people, and readiness for social interaction in the world.
A big thank you to science and mothers for proving what we already know--that the values in life can be taught to a child “through a mother's eyes,” setting the course for proper interaction for life skills and relationships.
References:
1. Kate Yandell, Proceedings of the Royal Society B ,04/10/2013.
2. Maxson J.McDowell, Biological Theory, MIT Press, 05/04/2011.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Parkinson’s disease is a progressive degenerative condition of the neurological system. The majority of Parkinson’s effects are on movement, often starting off very slowly and subtly. One of the earliest symptoms is a slight tremor in one or both hands. Other early symptoms include a lack of facial expression and decreased blinking of the eyes, so it looks like the person is always staring.
The next stage usually results in difficulty with initiating movement, especially walking. It frequently looks like it takes a tremendous concentrated effort to initiate walking and the steps often start off very small with a shuffling of the feet. At the same time, the disease stiffens the muscles of the arms so that when the person is walking there is a noticeable decrease in the swinging of the arms. Speech becomes much softer and writing becomes more of an effort, with handwriting getting smaller and smaller as the disease progresses.
Parkinson’s can also affect your visual performance, mainly in two parts of your eyes: the tear film and the ocular muscles.
It affects your tear film because of the decreased rate of blinking. The tear film is an important component of your optical system. It coats the surface of the cornea and if it is not smooth and uniform the result is a blurring of your vision. Blinking helps refresh your tear film and spreads it out uniformly. It is analogous to the washers and wipers on your car. If the windshield (like your cornea) is spotty you have a hard time seeing through that windshield. Turn on the washers and now there is more moisture on the surface but that is also spotty and hard to see through until the wipers go by and spread the moisture out evenly. That is very similar to how your cornea, tear film and your eyelids blinking interact to keep your vision clear.
If you don’t blink enough, the tear film begins to dry out in spots and having dry spots next to moist spots results in an irregular film and therefore blurred vision. That is how the decreased blinking frequency in people with Parkinson’s disease results in a complaint of intermittent blurred vision.
The other way the disease affects your vision is by creating a problem called convergence insufficiency. When you read, your two eyes turn inward toward each other in a process called convergence. Your eye muscles are activated in order to have the two eyes point inward to focus on the near object. By interfering with the interaction between your nerves and muscles, Parkinson’s makes it difficult to both initiate and sustain the convergence you need to keep both eyes focused on a near object.
This sometimes results in a disconnect between what a person is capable of reading on an eye chart for a short period of time and what happens after trying to sustain the effort over a longer period of time. This disconnect can result in some frustration. Often during an exam, a quick look at the distance eye chart allows the patient to see fairly well because the dry eye may not be causing any blurring if the patient just blinked a few times before reading the chart. A patient may also do well on the near chart because they are often being tested one eye at a time. When you read things up close with just one eye there is no need for the eyes to converge so they do well one eye at a time.
There are some other less-frequent eye problems that can occur with Parkinson’s. One is called blepharospasm, where the eyelids on either one side or both forcefully close involuntarily. A person can also end up with a condition called apraxia of eye opening, where they can’t voluntarily open the eyelids. This is different from blepharospasm because in this condition the lids are not being forcefully closed, they just won’t open when you want them to.
The majority of these problems do improve if the Parkinson’s is treated with medication or even brain stimulation.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided on this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Have you ever felt a twitching sensation in your eye? Did it feel like everyone was looking at you because of it? Were you worried that it was the beginning of a big problem?
Relax--it’s not likely to be a big deal. Most of the time it is not even visible to other people.
It's reassuring to know it’s almost never your actual eyeball that is twitching; it’s your eyelid muscle. Actual eye twitching is fairly rare and your vision would be pretty blurry if that's what were really happening.
The eyelid has a muscle in it that closes the eyelid and that muscle has a very high concentration of innervation. Because of that dense nerve tissue in the eyelid, anything that makes your nervous system a little hyped up or off kilter can result in the eyelid twitching.
What are some of the risk factors for eyelid twitching?
Fatigue
Not getting enough sleep can result in your nervous system not performing at its best and one of the results may include eyelid twitching. If you are getting frequent eyelid twitching, try to make sure you are getting the proper amount of sleep.
Caffeine
Too much caffeine can certainly overexcite your nervous system and result in frequent eyelid twitching. If twitching is becoming something you experience frequently, it might be time to cut down your caffeine intake. While coffee tends to be the biggest offender, caffeine does come in other flavors. Tea, colas, and chocolate are other common ones. Other items that you don’t think of as much: ice cream (especially chocolate or coffee flavors), de-caffeinated coffee (still has some caffeine), power or energy bars, non-cola soft drinks (Mountain Dew, Dr. Pepper, some root beers) and some OTC pain relievers (Excedrin Migraine, Midol Complete, and Anacin).
Stress
This is a hard one to quantify but if I ask most people who come to me with eyelid twitching if they are under more stress than usual the answer is almost always, "YES!" This is not an easy thing to mitigate. You may need to seek some help from your internist or psychiatrist or you could try some home remedies like long baths or whatever helps you relax.
Dry Eyes
One of the first things I tell people suffering from eyelid twitching is to use a lubrication drop in their eye. Anything that irritates your eye may result in eyelid twitching and an OTC lubricating drop in the eye might decrease the eyelid twitching. It is certainly worth a try.
What if the twitching won’t go away? Could it be anything more serious?
There is a condition called essential blepharospasm that could cause frequent twitching of the eyelid. In this condition you don’t just feel the lid twitching, but the entire eye starts closing involuntarily like you are trying to wink at someone. This can start to interfere with your normal daily life and can make things like driving and reading difficult to do. If the lid closing gets that significant, the main treatment for it is Botox injection to weaken the muscle that closes the eyelids. This stops the lid twitching very effectively, but it often needs to be repeated every 3 or 4 months.
Most of the time, eyelid twitching just goes away on its own as mysteriously as it came. If you experience twitching that doesn’t go away, try making some of the modifications I mention above and if that doesn’t work you should schedule an exam.
Article contributed by Dr. Brian Wnorowski, M.D.
A wrinkle on the retina -- which is also known as an epiretinal membrane (ERM) or a macular pucker -- is a thin, translucent tissue that develops on the surface of the retina.
The retina is the inner layer that lines the inside of the back of the eye and is responsible for converting the light image into an electrical impulse that is then transmitted to the brain. An epiretinal membrane that forms on the retina goes unnoticed by the patient many times, and is only noticed during a dilated eye exam by an eye doctor.
Epiretinal membranes can become problematic if they are overlying the macula, which is the part of the retina that is used for sharp central vision. When they become problematic they can cause distortion of your vision, causing objects that are normally straight to look wavy or crooked.
Causes of a wrinkle on the retina
The most common cause is age-related due to a posterior vitreous detachment, which is the separation of the vitreous gel from the retina. The vitreous gel is what gives the eye its shape, and it occupies the space between the lens and the retina. When the vitreous gel separates from the retina, this can release cells onto the retina's surface, which can grow and form a membrane on the macula, leading to an epiretinal membrane.
ERMs can also be associated with prior retinal tears or detachments, prior eye trauma, or eye inflammation. These processes can also release cells onto the retina, causing a membrane to form.
Risk factors
Risk for ERMs increases with age, and males and females are equally affected.
Both eyes have ERMs in 10-20% of cases.
Diagnostic testing
Most ERMs can be detected on a routine dilated eye exam.
An optical coherence tomography (OCT) is a noninvasive test that takes a picture of the back of the eye. It can detect and monitor the progression of the ERM over time.
Treatment and prognosis
Since most ERMs are asymptomatic, no treatment is necessary. However, if there is significant visual distortion from the ERM or significant progression of the membrane over time, then surgical intervention is recommended. There are no eye drops, medications, or nutritional supplements to treat or reverse an ERM.
The surgery is called a vitrectomy with membrane peeling. The vitrectomy removes the vitreous gel and replaces it with a saline solution. The epiretinal membrane is then peeled off the surface of the retina with forceps.
Surgery has a good success rate and patients in general have less distortion after surgery.
Article contributed by Dr. Jane Pan
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Demodex folliculorum -- often just called demodex -- is a mite that occurs naturally on many people's faces and resides in hair follicles, particularly the follicles of eyelashes. Most of the time, these mites cause no problems whatsoever. However, sometimes an infestation can become particularly parasitic, resulting in unhealthy eyelid margins and leading to problems. Those problems as a group are called blepharitis. Blepharitis can be caused by caused by several things, including allergies, bacterial overgrowth, Rosacea and also by demodex.
Often, diagnosis of mite infestation by your eye doctor can be difficult. The symptoms can mimic other causes of blepharitis, which is one of the most prevalent diseases we see.
The most common sign of a demodex infestation is a cylindrical cuff or "sleeve" at the base of the eyelash. Symptoms include redness, itching, burning, dry eyes and general discomfort in the eyelid.
The probability of demodex infestation increases gradually with age, with nearly 100% of people having demodex in their eyelashes after age 70. If there are no symptoms present, nothing needs to be done about demodex, as it is a natural occurence. If any of the before-mentioned symptoms are present, however, eyelid hygiene with tea tree oil is usually the first line treatment. Tea tree oil is known to kill the mites and there are now several brands of “eye lid scrubs” that come with tea tree oil in them.
There are also often in-office methods available for exfoliating eyelids.
If you're experiencing any demodex symptoms, make an appointment to see what treatment might be right for you.
Article contributed by Dr. Jonathan Gerard, O.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Here are 11 bad contact lens habits we eye doctors often see--
#1 Sleeping in your contacts.
This is the No. 1 risk factor for corneal ulcers, which can lead to severe vision loss and the need for a corneal transplant. Your cornea needs oxygen from the atmosphere because it has no blood vessels. The cornea is already somewhat deprived of oxygen when you have your eyes closed all night, and adding a contact on top of that stresses the cornea out because of the lack of oxygen. You don’t need to see when you are sleeping! TAKE YOUR CONTACTS OUT! I promise your dreams will still look the same.
#2 Swimming in your contacts.
Salt, fresh, or pool water all have their individual issues with bacteria, amoeba, chemicals, etc., that can leach into your contacts. If you end up wearing them in the water, then take them out as soon as you are done and clean and disinfect them.
#3 Using tap water to clean contacts.
Tap water is not sterile. See No. 2.
#4 Using your contacts past their replacement schedule.
The three main schedules now are daily, two weeks, and monthly. Dailies are just that – use them one time and then throw them away. They are not designed to be removed and re-used. Two-week contacts are designed to be thrown away after two weeks because they get protein buildup on them that doesn’t come off with regular cleaning. Monthly replacement contacts need to have both daily cleaning and weekly enzymatic cleaning to take the protein buildup off. Using your lenses outside of these wearing and maintenance schedules increases the risk of infection and irritation.
#5 Getting contacts from an unlicensed source.
Costume shops and novelty stores sometimes illegally sell lenses. If you didn’t get the fit of the lenses checked by an eye doctor, they could cause serious damage if they don’t fit correctly.
#6 Wearing contacts past their expiration date.
You can’t be sure of the sterility of the contact past its expiration date. As cheap as contacts are now, don’t take the risk with an expired one.
#7 Topping off your contact lens case solution instead of changing it.
This is a really bad idea. Old disinfecting solution no longer kills the bacteria and can lead to resistant bacteria growing in your case and on your lenses that even fresh disinfecting solution may not kill. Throw out the solution in the case EVERY DAY!
#8 Not properly washing your hands before inserting or removing contacts.
It should be self-evident why this is a problem.
#9 Not rubbing your contact lens when cleaning, even with a “no rub” solution.
Rubbing the lens helps get the bacteria off. Is the three seconds it takes to rub the lens really that hard? “No rub” should never have made it to market.
#10 Sticking your contacts in your mouth to wet them.
Yes, people actually do this. Do you know the number of bacteria that reside in the human mouth? Don’t do it.
#11 Not having a backup pair of glasses.
This is one of my biggest pet peeves with contact lens wearers. In my 25 years of being an eye doctor, the people who consistently get in the biggest trouble with their contacts are the ones who sleep in them and don’t have a backup pair of glasses. So when an eye is red and irritated they keep sticking that contact lens in because it is the only way they can see. BAD IDEA. If your eye is red and irritated don’t stick the contact back in; it’s the worst thing you can do!
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

There are many options available to adults and children for corrective lenses (glasses and contacts) when engaged in physical activities.
Here is a look at the different modalities and the pros and cons of each:
Prescription Sports Goggles (e.g., Rec Specs)
The main benefits of goggles while playing sports are vision stability and eye protection. When playing fast-moving sports--like basketball, soccer, and rugby--elbows, wrists, and heads fly around at high speed, increasing the risk of eye injury. The eyes and eye sockets can be protected when covered by shatter-proof lenses. Additionally, there is no worry over having a contact lens pop out of the eye, which can be a debilitating experience for some people. The main drawback to goggles is that they can be cumbersome, decrease peripheral vision, and fog up. Additionally, very high prescriptions might not be available due to frame limitations. On the whole, this is a very good option for many people. One additional advantage to sports goggles is that they can often be made with Transitions lenses, providing automatic sun protection in bright light.
Contact Lenses
For many people, the best visual option is contact lenses, particularly soft contact lenses. The main benefits include no decrease in visual field, no fogging of lenses, and no unsightly, heavy glasses. But where sports goggles shine, contact lenses fall short--there is a higher risk of injury, the possibility of less stable vision (especially when wearing multifocal or astigmatic lenses), and the potential of a lens falling out during activities. Gas permeable (hard) lenses are not recommended for sports.
Wearing Nothing
For those whose prescriptions are not so high as to prevent proper functioning without correction, wearing no correction whatsoever is a fine choice. I’m often asked by parents whether their child absolutely needs to wear correction when they are playing sports. It really depends on how high the prescription is and the activity in which the child is engaged. If someone can see well enough to perform the goals without being hindered, not wearing any correction is perfectly fine.
There are plenty of options available for athletes. Visit your eye doctor to see what the best option is for your particular needs.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Oftentimes, contact lens wearers will skimp on their lens care because some of the solutions are costly and it seems like a good way to save some hard-earned cash. But this is not a good idea.
Cutting corners can result in infections or irritations, and after one or two copays to your eye doctor's office you probably will have spent more than what you saved in a year by cutting corners--plus you have to deal with your discomfort and inability to wear your contact lenses while you are being treated.
The reasons you clean your contacts is to give increased lens comfort, prolong lens oxygen permeability, and to protect your eyes from infection. The reason you have to disinfect your contact lenses is - as nasty as it may sound - that your eyeball and eyelids are covered in essential bacteria that are kept in check by your body’s immune system. When you remove your contact lens at night it is covered in these essential bacteria. If you don't kill them overnight this will allow the bacteria to grow unchecked and then, instead of inserting a freshly cleaned lens, you are inserting a lens covered in more bacteria than your eye is used to and you end up getting an infection.
Let’s talk about the most widely used type of solution - the multipurpose solution. While this is often the most incorrectly used solution, multipurpose solution is a very safe and effective disinfection method when used properly.
Many multipurpose solutions advertise themselves as “No Rub.” Just put it in the case and you are done. This is OK to do, but a quick rub with the no-rub solution in the palm of your hand and the opposite hand’s middle or ring finger provide an even better cleaning option. Just the slight roughness of your fingerprint adds a light scrubbing effect that helps improve the removal of surface debris, protein, and mucous better than just letting the lens soak overnight. This rubbing of the lens is especially important for women to remove any cosmetics that are rarely removed by just soaking alone. These few seconds of extra cleaning will make your lenses stay more comfortable longer during their wearing cycle, and help to keep the pores of the lenses open, allowing more oxygen to contact your cornea.
Many name brands and store/warehouse brands of multipurpose solutions exist. All are FDA approved to do the same thing: clean/disinfect/rinse/store your contact lenses. You can't really mess them up unless you try. Remove the lenses, lightly rub them with the multipurpose solution, place your lens into a CLEAN and DRY lens case, and cover the lens with solution to disinfect it. Then let it sit for the number of hours recommended by the manufacturer, generally between 4 to 8 hours, or overnight. Remove the lenses in the morning, rinse with the same multipurpose solution and rinse the lens case out and leave it open to air dry in an area away from your sink and toilet to prevent airborne contaminants from getting into your case as it dries.
The biggest misuse of the multipurpose solution is not changing your case’s solution nightly and just adding more solution to the case each night. We call this “topping off the case.” This is NOT safe because it will lose disinfection power since the old/used solution was busy killing the bacteria and organisms from the night before. Just adding a little fresh solution will eventually allow for the bacteria to take over and you may be adding more bacteria into your eyes than if you never disinfected the lenses to begin with.
Multipurpose solution companies oftentimes will give you a new case when you buy bigger bottles of solution. You should start using the new case with the new bottle of solution. Dont's just stash the case away. There are fungi and other organisms that have been demonstrated to grow from very old lens cases so USE the new case and don't keep it for when you break the old one.
There are many different multipurpose solutions on the market. They aren't cheap and it is tempting to purchase “what is on sale” to save a few dollars. If it does the same thing as the expensive one, then why bother spending the extra? But remember, your contacts are like little sponges that soak up your lens solution. The lens companies don't care if brand A’s solution is compatible with brand B’s or C’s. So over time you can develop a sensitivity to one particular brand of solution, or mixing solutions with the same lens can cause a chemical reaction that occurs because the solutions are not compatible. If you are using the same brand regularly and start having issues your doctor may recommend a solution change to another company that you haven't tried and this may potentially solve your problem. But if you have used several different ones in a few weeks prior to your visit it makes it much harder to determine the cause of your irritation.
The generic/store brands are usually fine products but a grocery store or discount chain doesn’t have a factory that makes their solution for them--they purchase it from a larger supplier. These third-party suppliers can alter their recipe for their multipurpose lens solution and you as the consumer would never know. You could just start finding your contacts are not as comfortable as they used to be and it is actually the unknown generic solution change that is bothering you. Brand name companies like Bausch and Lomb, AMO, and Alcon will rarely make product changes without making consumers aware that they've reformulated the product so if something changes with the reformulated product you have a better chance of knowing it than with a generic solution manufacturer.
Finally, there is a product called saline solution. Saline is extremely inexpensive, generally half to a third the price of multipurpose solutions. This is a product made by many different companies and was the first lens solution ever used. Saline solution was initially used in a heat disinfection system where the lenses were boiled nightly. The boiling of the lens provided the disinfection, not the saline solution. The solution was to just to prevent the lens from drying out while you cooked it. You should NEVER use saline solution as a replacement for multipurpose solution. Saline solution is NOT a disinfectant for your lenses. It doesn’t contain an agent that will prevent bacteria and organisms from growing in the case overnight. However, it’s totally acceptable if you want to rinse your lenses in the morning with saline prior to inserting them after they were disinfected with your multipurpose solution.
Oftentimes, a practitioner will recommend a certain type of solution to help with things like dryness, environmental allergies, or allergies to specific solutions. I always recommend to check with your practitioner before making any changes to your lens care solution or lens care routine. The best advice for saving money on your preferred solution is buy extra when it is on sale, buy in bulk, and buy what is most comfortable in a multipurpose solution for you. Then stick with it and use it correctly for many years of happy lens wear.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
Hydroxychloroquine (Plaquenil) was originally used to treat malaria and is now commonly used to treat rheumatological and dermatological diseases. It is frequently used for rheumatoid arthritis (RA) and Lupus and is often very effective in mitigating the joint and arthritic symptoms these diseases can cause.
One of the most significant side effects of the drug is its possibility of causing eye problems resulting in blurred or decreased vision. The most common issue is damage to the retina. It can impair color vision or damage the retinal cells, particularly in the area right around the central vision.
In your retina, the area that you use to look straight at an object is called the fovea. The fovea is the area that provides you with the most definition when looking at an object. The area just around the fovea is called the macula and it has the ability to see objects with slightly less definition than the fovea but significantly better than the rest of your retina, which accounts for your peripheral vision. The most common place for Hydroxychloroquine to cause a problem is in a ring of the macula surrounding the fovea.
The reason it is important to detect any of these changes as early as possible is because in many instances the changes are not reversible even if you come off the medication.
The risk of this happening is highly correlated with the cumulative dose of the drug you have received. So, the higher the dose and the longer you have been on it the higher your risk.
The current recommendation is a daily dose that does not exceed 6.5 mg/kg/day (that is milligrams per kilograms per day). There are approximately 2.2 pounds in a kilogram. The pills come in 200 mg tablets. Most people who are on this drug are on either 200 mg once a day or 200 mg twice a day. The safety break point comes at around 135 pounds. People weighing more than that will stay within the safety guidelines (not more than 6.5mg/kg/day) at 400mg per day, but people under 135 pounds should probably only be taking 200 mg per day.
Other risk factors for Hydroxychloroquine retinal toxicity include kidney or liver disease and obesity. Obesity is a risk factor because the drug does not penetrate fat tissue so there is more of the drug in your lean body mass (including your retina and its supporting cells called the retinal pigment epithelium). What that means in real terms is that if you take two people who each weigh 140 pounds and put them both on 400 mg a day and one person is 4-foot 11 and the other is 5-foot 9, the 4-foot 11 inch person is at greater risk for side effects because the shorter person has more of their body weight in fat tissue. Since the hydroxychloroquine can’t penetrate the fat tissue that means there is a higher concentration of it in sensitive tissues like the retina. People with kidney and liver problems have a tougher time eliminating the drug from their system so they are at higher risk because the body is going to retain more of the drug for a longer period of time.
The recommendation is to have a baseline eye exam with dilation and a visual field test before or soon after starting the drug. A repeat of that exam should occur every year if there is no evidence of toxicity.
The actual incidence of retinal toxicity from hydroxychloroquine is difficult to pin down because there is usually a long time between being started on the drug and the start of any identifiable retinal toxicity. The overall rate of probable retinal toxicity is in the range of 1 of every 200 people treated. The rate is much lower than that in the first 7 years of treatment but gets to about 5 times higher after 7 years of treatment. Some of that data is old now and there is much greater awareness currently about keeping people below that 6.5 mg/kg/day dosage level.
I have been in practice for over 25 years and have seen “probable” retinal toxicity from hydroxychloroquine a total of 5 times and only once in the last 10 years when people have been more careful about keeping the dosage in the right range.
The drug can be very effective in its treatment of RA and Lupus and the likelihood of serious vision problems is small and can potentially be avoided with the correct dosing and monitoring of the eyes. Other drugs in the treatment for RA or lupus may have more frequent or serious side effects then Hydroxychloroquine so it would be wise to consider it a viable treatment option and not easily dismiss it because of the risk of what amounts to a fairly infrequent eye issue.
Article contributed by Dr. Brian Wnorowski, M.D.

In honor of St. Patrick’s Day and the “wearin’ of the green,” we thought it would be fun and fitting to share some interesting facts about green…eyes!
#1
Green is the rarest eye color. If your sparklers are truly green, you are something of a unicorn… only about 2% of the world’s population sport this hue.
#2
Green-eyed people can be found all around the globe. There is a Chinese village, Liqian, where a high percentage of the population sports green eyes and lighter hair.
#3
There isn’t any actual green pigment in a green eye. Melanin, a natural pigment that helps determine our skin, hair, and eye color, is found in all eyes. Brown eyes have quite a lot and blue eyes have relatively little. Green eyes are also low on melanin, but in addition they contain lipochrome, a yellowish, fat-soluble pigment. Lipochrome is also found in things like butter, eggs, and corn. So a little melanin, some lipochrome, and a cool light dispersing scattering called the Tyndall Effect combine to produce those rare green eyes!
#4
At least 16 genes contribute to eye color. You might have been taught in biology class that two brown-eyed parents can have only brown-eyed children, but it’s more complicated than that.
#5
Green eyes are popular in cultural references. Here are some famous characters with green eyes:
· Jane Eyre—that plucky governess living in a “haunted” mansion, from the book Jane Eyre
· Rapunzel—another courageous hero in Tangled
· Scarlet O’Hara—feisty protagonist in Gone with the Wind
· Scar—the scheming uncle in The Lion King
· Mary Jane Watson, Catwoman, Batgirl—green eyes are popular in the world of comics
· Sara Crewe—brave little girl from A Little Princess
· Harry Potter – from the Harry Potter book series by J.K. Rowling
#6
In a large survey performed by All About Vision, green was voted the most attractive eye color, with over 20% of the 66,000 respondents choosing this hue.
#7
More women than men have green eyes. Scientists aren’t sure why this is, but it suggests there is an underlying gender-related factor that causes this difference.
#8
 Animals can also sport green eyes. Green eyes occur in dogs, snakes, frogs, birds, monkeys, multiple members of the cat family, and many other animals.
Animals can also sport green eyes. Green eyes occur in dogs, snakes, frogs, birds, monkeys, multiple members of the cat family, and many other animals.
#9
People with green eyes are more likely to have certain health issues. Green eyes are more prone to melanoma of the uvea, a type of eye cancer, than are dark eyes. The same is true for macular degeneration. If you have green eyes, protect those beautiful peepers with a quality pair of sunglasses to lower your chances for these diseases!

Now that you have picked up your new pair of prescription eyeglasses, your focus becomes taking care of them. This is a task many disregard, but it is absolutely imperative that you make sure you are following a couple simple steps to keep the quality of your vision with your new spectacles.
We are all guilty of using a garment when in a rush to wipe away a pesky smudge on our glasses. This act is unfortunately the worst thing you can do for your lenses.
No matter how clean your clothes are, dust particles and even small bits of sand and debris cling to them. Since eyeglass lenses are not made of diamonds, these tiny little particles can do tremendous amounts of damage to your new lenses. The smallest little crumb can grind a scratch directly in your line of vision, which in turn can render your glasses almost useless.
Most of us know what it feels like trying to concentrate on the world in front of you when there is a little scratch distorting and distracting your vision. A majority of the time, these little scratches can be avoided by following a few simple steps.
You may have noticed while shopping in your favorite store that they sell a variety of eyeglass cleaners. You need to be careful because the sprays and wipes which you can purchase in retail stores are not necessarily approved for all types of eyeglass lens materials.
This factor makes them fall under that category of products that many eye care professions cannot recommend. Most of these liquids contain a form of acetone or other cleaning agent that is too harsh for plastic lenses. Many years ago, when all eyeglasses were actually made out of crown glass, these products would have worked just fine. Now, during a time with thinner, lighter materials like cr-39 plastic and polycarbonate, these products have proven to be too hard on the lenses.
Over time, the lenses will start to break down if exposed to the chemicals used in these sprays, causing a fogging effect. Once again, you are left with a pair of glasses that are now unable to be used.
Now that we have gone over the two main culprits in the destruction of eyeglass lenses, other than accidents, let’s focus on some tips to extend the life of your glasses.
Most importantly, you should use an eyeglass case. For the large portion of patients who wear their glasses all day, it’s understandable how awkward it can be to carry a case around. But it’s nowhere near as frustrating as realizing the new pair of eyeglasses you just purchased is becoming scratched and ruined.
Also, you do not need to carry the case with you everywhere you go. Strategically leaving a case on a bedside table, in your car, or in a purse is the difference between “life or death” for your glasses.
There is also a simple way to clean your glasses that does not require you to purchase anything you probably don’t already have at home. Using lukewarm water at the sink, place a small, pea-sized dab of dish soap on your fingers. Gently rub the soap on both lenses from side to side, and then rinse with warm water. A disposable paper towel is recommended to dry the glasses.
Disposable towels work because they are just that, disposable - which guarantees they are not carrying dirt or sand from a prior use.
Taking care of your glasses today means you have them for clear vision tomorrow and into the future.
Article contributed by Richard Striffolino Jr.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
As an eye doctor, diagnosing a red eye can be challenging. Are we dealing with an infection, allergy, inflammation, or dryness?
A common question we get is, “Doc, my eyes are red, burning, itchy, and tearing. Is this dry eye or from allergies?” The short answer is it could be one, both, or neither. We'll outline various ways these conditions present clinically and the treatments for them.
The hallmark symptom of allergy – meaning if you have this symptom you almost definitely have the condition – is itching. Red, watery, ITCHY eyes are almost invariably due to an allergen, whether environmental or medicinal. It is one of the most common ocular conditions that we, as eye doctors, treat -- especially when plants are filling the air with pollen as they bloom in the Spring and then die off in the Fall.
The itching occurs because an immune cell called a mast cell releases histamine, causing the itching sensation. It can be quite unbearable for the sufferer, causing them to rub their eyes constantly, which actually increases the amount of histamine in the eye, leading to worsening of the symptoms.
Treatments may include:
- Over-the-counter or prescription allergy drops (mostly anti-histamines or mast cell stabilizers).
- Topical steroids (to get the inflammation under control).
- Cool compresses applied to the eye.
Patients sometimes need to take drops every day to keep their symptoms under control.
Dry eye can have many of the same symptoms as allergic eye disease, with the eye being red and possibly watery ("My eyes are tearing--how could it be dry eyes?"). The main exceptions are that people with dry eyes tend to complain more of burning and a foreign body sensation - like there is sand or gravel in the eye - rather than of itchiness.
Dry eye is a multi-faceted disease with many different causes and treatments. Treatment ranges from simple re-wetting eye drops to long-term medications (both topical and oral), as well as non-medicinal treatments such as eyelid heating treatments.
So how do we determine the difference? The first question I ask patients who complain of red, watery, uncomfortable eyes is, “What is your MAIN symptom? Itching or burning?” The answer will likely direct which course of treatment we take, and as those treatments sometimes overlap, you may have a component of both dry eye and allergy.
That is important to distinguish because many of the treatments we use for allergies - like antihistamine eye drops - can sometimes make the dryness worse. Though neither of these conditions is 100% curable (except maybe for allergy, where if you remove the allergen, you obviously won’t get symptoms!). We have many tools in our treatment arsenal to keep the symptoms at bay.
Unfortunately, dry eye and allergy aren’t the only two things that can cause your eye to have the multiple symptoms of red, watery, itchy, burning eyes. There are other problems, such as blepharitis, that can produce a similar appearance, as well as bacterial and viral infections.
So before embarking on a particular therapy, it is wise to have a good exam to help you get on the right track of improving your symptoms.
Article contributed by Dr. Jonathan Gerard
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

"It was the best of times, it was the worst of times." These famous words by Charles Dickens are playing out today in the area of technology.
We are living in the best of times when it comes to obtaining knowledge at the push of a button. But smartphones, laptops, video games, tablets, etc., can really increase our daily total screen time.
What are the symptoms of too much screen time for the eye, and how can you combat these symptoms? Research shows that screen time can adversely affect your eyes, focus, moods, and ability to sleep and relax.
Doctors are also seeing an increase in dry eye syndrome because patients do not blink often enough while they are staring at the screen for a prolonged period of time. The lack of blinking can cause burning or watery eyes, rubbing of the eyes, and frequent headaches.
The key to combatting these symptoms is to consciously blink more, use rewetting eye drops, and take frequent breaks. Make it a priority to practice the 20-20-20 rule. For every 20 minutes of screen time, take a 20 second break, focusing on a target 20 feet away. Your eye doctor might also recommend specialized computer lenses with anti-glare properties to minimize fatigue.
Lots of screen time seems to be especially bad for children, especially young ones. Pediatricians often advise no screen time for those 2 and younger, and just 1-2 hours per day for older children. In addition to other physical and mental health issues caused by too much screen time, there seems to be a higher incidence of myopia in children that spend a lot of time with digital devices.
It is important to reiterate that screen time is not bad if used with moderation and frequent breaks. In fact, many computer programs are used to help patients strengthen their eye muscles and promote hand eye coordination.
So take frequent breaks, use preventative measures (such as re-wetting eye drops, anti-glare computer lenses, and eye exercises), and keep children engaged with the non-digital world as much as possible. Your eyes, and the eyes of those you love, will thank you!
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
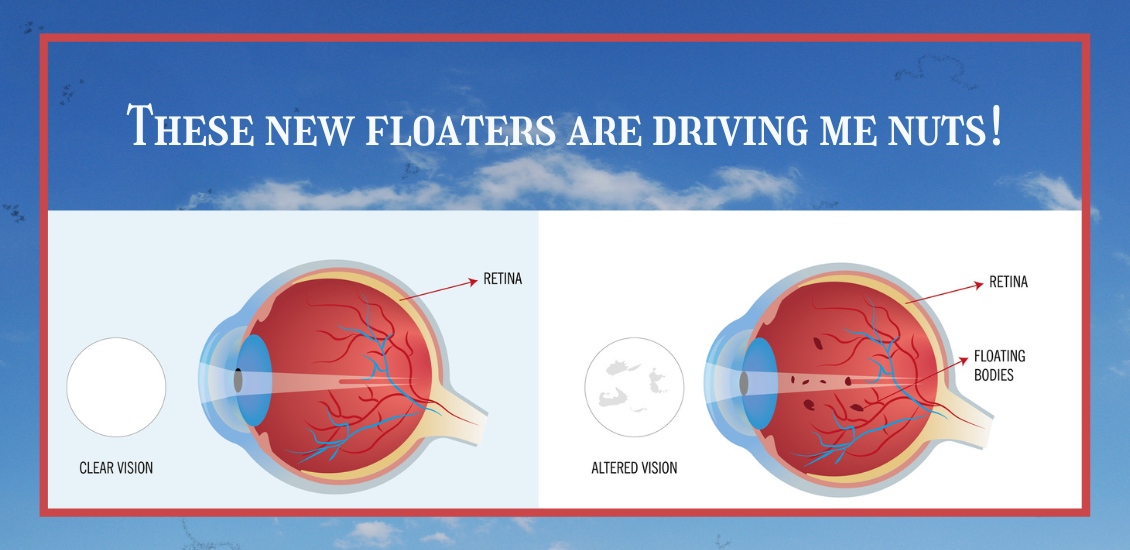
Do you have floaters in your vision?
Floaters are caused by thick areas in the gel-like fluid that fills the back cavity of your eye, called the vitreous.
Many people, especially highly near-sighted people, often see some degree of floaters for a good portion of their lives. Often, these floaters are in the periphery of your vision and may only be visible in certain lighting conditions. The most frequent conditions are when you are in bright sunlight and are looking toward the clear blue sky. I know this from personal experience since I have a floater in my left eye that I most often see when swimming outdoors. Every time I turn my head to the left to breathe I see this floater moving in my peripheral vision.
This is totally harmless other than when I’m swimming in the ocean and swear that sudden object in my peripheral vision is a shark bearing down on me. Some people who have floaters are not as lucky-- the floater might be in their central vision and almost constantly annoying, especially when trying to read.
The second scenario in which floaters occur is during the normal aging process. The vitreous gel in the back of the eye starts to shrink as we age and at some point it collapses in on itself and pulls away from the retina. This sometimes results in a sudden set of new floaters.
When that happens you need to be checked for signs of a retinal tear or detachment. As long as your retina survives that episode without any problems, the floaters themselves may stick around for a while and can be rather annoying.
Most people eventually adapt to the floaters; the brain learns to filter them out so you are no longer aware of them. The vitreous can also collapse more as time goes on and the dense floater you are seeing initially may move further forward and drop lower in the eye so the shadow it is casting is less intense and more in the periphery of your vision where it is much easier to ignore.
The first line of treatment for floaters has been, and still is, to learn to live with them. Once you have your retina checked and there is nothing wrong there, the floaters themselves are harmless and will not lead to any further deterioration of your vision--which is why, if at all possible, you should just live with them. This is especially true if the floaters are new because the overwhelming majority of people with new floaters will eventually get to the point where they are no longer seeing them or at least where they are not interfering with normal daily activities.
If you have tried to wait them out and live with them but they are still interfering with your normal daily activities, you may want to consider having them treated with a laser.
This treatment is newer and involves using a special laser to try to break down large floaters into much smaller pieces that may no longer be visible. In a study of the laser treatment involving 52 patients, 36 were treated with the laser (a single laser treatment session) and 16 people had a sham treatment (meaning they went through everything the treated group did but did not actually have the real treatment done). In the people who were actually treated, 54% reported a significant improvement in the floater symptoms while 0% in the sham group reported any improvement (no placebo effect). There were no significant side effects in either group.
Some points to note in the above study:
54% of people treated noted a significant improvement in their floater symptoms with a single treatment. That’s clearly not anywhere near a guaranteed improvement.
Other people have noted an improvement after more than one session, bringing the total expected improvement into the 70% range, with one or more treatments.
Another point to note is that there were no significant side effects to the treatment.
Although true in this small study, it does not mean that there are no risks to the laser treatment. Although rare, there have been reports of damage to the retina, optic nerve, or the lens of the eye.
Another treatment that can be used to treat floaters is a surgical procedure called a vitrectomy. This involves surgically going inside the back of the eye and removing the vitreous. This surgical procedure carries a higher risk than the laser treatment and is not 100% effective.
In summary, laser treatment is a good addition to the tools to deal with significant floater problems. If you have floaters for at least six months and they are central and interfering with your normal daily activities and you want to see if this laser treatment could be right for you, check with your eye doctor.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.
One of the hardest questions eye care professionals routinely have to deal with is when to tell people with visual difficulaties that they need to stop driving.
Giving up your driving privilege is difficult to come to terms with if you have a problem that leads to permanent visual decline.
The legal requirements for visual acuity vary from state to state. For example, in New Jersey the legal requirement to drive, based on vision, has been 20/50 vision or better with best correction in one eye for a “pleasure” driving license. For a commercial driving license, the requirement is 20/40 vision or better in both eyes.
In some states there is also a requirement for a certain degree of visual field (the ability to see off to the sides).
According to the Insurance Institute for Highway Safety, the highest rate of motor vehicle deaths per mile driven is in the age group of 75 and older (yes, even higher than teenagers). Much of this increased rate could be attributable to declining vision. There are also other contributing factors, such as slower reaction times and increased fragility, but the fact remains that the fatality rate is higher. , And so, when vision problems begin to occur with aging it is extremely important to do what is necessary to try to keep your vision as good as possible.
That means getting regular eye exams, keeping your glasses up-to-date, dealing with cataracts when appropriate, and staying on top of other vision-threatening conditions such as macular degeneration, glaucoma, and diabetes.
It is our responsibility to inform you when you are no longer passing the legal requirement to drive. Although not all states have mandatory reporting laws, your eye doctor will record in your medical record that you were informed that your vision did not pass the state requirements to maintain your privilege. And, yes, it is a privilege -- not a right -- to drive.
If you have a significant visual problem and your vision is beginning to decline, you need to have a frank discussion with your eye doctor about your driving capability. If you are getting close to failing the requirement, you need to start preparing with family and loved ones about how you are going to deal with not being able to drive.
Many of us eye doctors have had the unfortunate occurrence of having instructed a patient to stop driving because of failing vision, only to have him ignore that advice and get in an accident. Don’t be that person. Be prepared, have a plan.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Eye doctors typically pride themselves on being able to improve someone’s vision through glasses or contact lens prescriptions. Whether it’s a first-time glasses wearer, or someone having either a small or large change in their prescription, we like to aim for that goal of 20/20 vision.
Despite our best efforts, however, correcting vision to 20/20 is not always a positive outcome for the patient. Whether someone will be able to tolerate their new prescription is based on something called neuroplasticity, which is what allows our brains to adapt to changes in our vision.
You or someone you know may have had this happen: Your vision is blurry, so you go to the eye doctor. The doctor gives you a new prescription, but when you get your new glasses, things seem “off.”
Common complaints are that the prescription feels too strong (or even too clear!) or that the wearer feels dizzy or faint. This is especially true with older patients who have had large changes in prescription, since neuroplasticity decreases with age. It is also more likely to happen when the new prescription has a change in the strength or the angle of astigmatism correction. Conversely, this happens less often in children, since their brains have a high amount of plasticity.
Quite often, giving the brain enough time to adapt to the new vision will decrease these symptoms.
Whenever a patient has a large change in prescription, I tell them that they should wear the glasses full time for at least one week. This is true for both large changes in prescription strength, as well as changing lens modality, e.g., single vision to progressives.
Despite the patient’s best efforts, though, sometimes allowing time to adapt to the new vision isn’t enough, and the prescription needs to be adjusted. Even when someone sees 20/20 on the eye chart with their new glasses, if they are uncomfortable in them even after trying to adjust for a week then we sometimes have to make a compromise and move the script back closer to their previous script so that there is less change and they can more easily adapt.
In conclusion, adapting to a new prescription can sometimes be frustrating. It does not mean there is anything wrong with you if you have difficulty adjusting to large changes in a prescription. With a little patience and understanding about how your brain adapts to these kinds of changes, your likelihood of success will be that much higher.
Article contributed by Dr. Jonathan Gerard
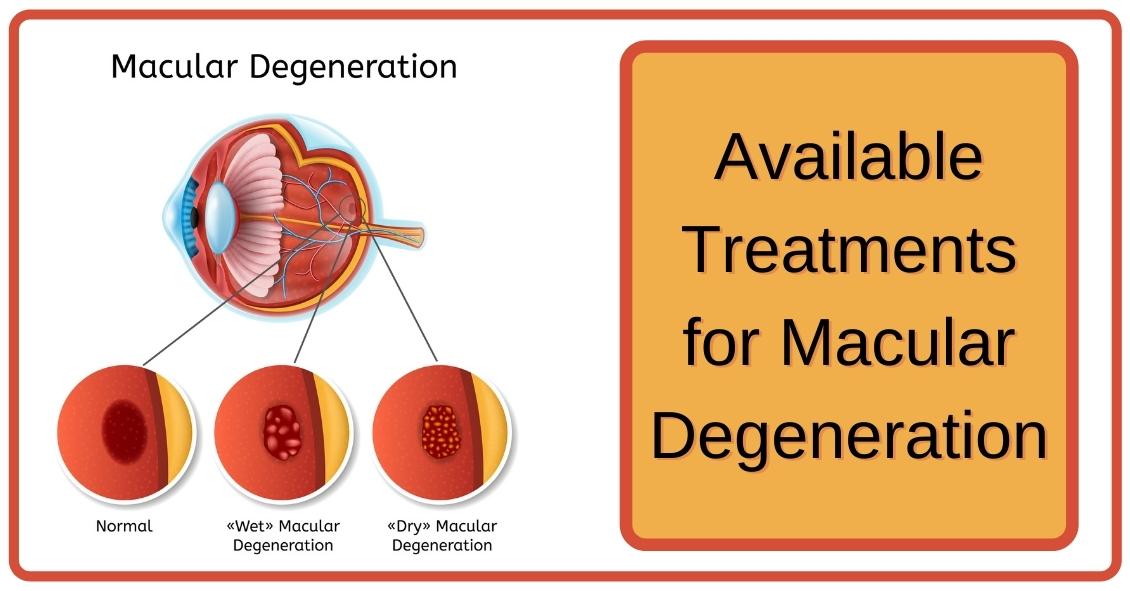
When confronted with a diagnosis of Age Related Macular Degeneration (AMD), it's natural to wonder what you should do. Here are some treatment options for both Dry and Wet Age Related Macular Degeneration.
Dry AMD Treatments
Nutrition Supplements
The Age-Related Eye Disease Study 2 (AREDS2) showed that people at high risk of developing advanced stages of AMD benefited from taking dietary supplements. Supplements lowered the risk of macular degeneration progression by 25 percent. These supplements did not benefit people with early AMD or people without AMD.
Following is the supplementation:
- Vitamin C - 500 mg
- Vitamin E - 400 IU
- Lutein – 10 mg
- Zeaxanthin – 2 mg
- Zinc Oxide – 80 mg
- Copper – 2 mg (to prevent copper deficiency that may be associated with taking high amount of zinc)
Another study showed a benefit in eating dark leafy greens and yellow, orange and other fruits and vegetables. These vitamins and minerals listed above are recommended in addition to a healthy, balanced diet.
It is important to remember that vitamin supplements are not a cure for AMD, nor will they restore vision. However, these supplements may help some people maintain their vision or slow the progression of the disease.
Wet AMD Treatments
Injection of Anti-VEGF
The most common treatment for wet AMD is an eye injection of anti-vascular endothelial growth factor (anti-VEGF). This treatment blocks the growth of abnormal blood vessels, slows their leakage of fluid, potentially helps slow vision loss, and in some cases, improves vision. There are multiple anti-VEGF drugs available: Avastin, Lucentis, and Eylea.
You may need monthly injections for a prolonged period of time for treatment of wet AMD.
Laser Treatment for Wet AMD
Some cases of wet AMD may benefit from thermal laser. This laser destroys the abnormal blood vessels in the eye to prevent leakage and bleeding in the retina. A scar forms where the laser is applied and may cause a blind spot that might be noticeable in your field of vision.
Photodynamic Therapy or PDT
Some patients with wet AMD might benefit from photodynamic therapy (PDT). A medication called Visudyne is injected into your arm and the drug is activated as it passes through the retina by shining a low-energy laser beam into your eye. Once the drug is activated by the light it produces a chemical reaction that destroys abnormal blood vessels in the retina. Sometimes a combination of laser treatments and injections of anti-VEGF mediations are employed to treat wet AMD.
Article contributed by Jane Pan M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.

Transition lenses in eyeglasses have been around for many years now. The mechanics behind transition lenses is that certain chemicals in the lens interact with UV light from the sun and turn the lenses dark when you go outside and back to clear when you go inside.
This is a great accompaniment to sunglasses, as it is not always convenient to be carrying around multiple pairs of glasses with you, especially when going from inside to outside frequently. However, there are some drawbacks to transitions, including the fact that they don’t get as dark as sunglasses, have some difficulty turning dark in the car, and have a tendency to keep a slight constant tint even in dark conditions.
Vistakon, the optical wing of Johnson & Johnson, came out with the first transition contact lens a few years ago. They work well for some people, and don't seem to do a lot for others.
Just a couple personal thoughts: It can look a little strange, depending on the person and the eye color. The material itself turns gray, and therefore the person can be walking around with eyes that look darker than normal. On the plus side, though, this would be good for people limited by high prescriptions and who have difficulty with peripheral vision and glasses, yet still want the transitioning technology. On the other hand, wearing clear contact lenses with sunglasses would provide better sun coverage with the ability to remove the sunglasses when desired.
An area where transition contacts might become very useful is in outdoor sports. For any athlete who is playing an outdoor sport where the lighting conditions may change from day to day or even within a single game or event, these contacts might significantly improve the ability to perform. This is especially true in any sport where there may be significant contact or rapid head movement that can make it difficult to compete in sunglasses.
While still in its infancy, transitioning contact lenses look to be a promising technology.
Article contributed by Dr. Jonathan Gerard
For over 40 years the standard surgical treatment for glaucoma was a procedure called a trabeculectomy.
In a trabeculectomy, the ophthalmic surgeon would make a hole in the wall of eye to allow fluid from the inside of the eye to flow out of the eye and then get resorbed by the blood vessels in the conjunctiva (the mucous membrane that covers the white part of the eye).
This surgery often resulted in a large decrease in the Intraocular Pressure (IOP). Reducing the IOP is the goal of glaucoma surgery because multiple studies show that if you can reduce the pressure the progression of glaucoma slows.
The problem with trabeculectomy is that although it frequently lowers the pressure, it also has a fairly high complication and/or failure rate. This led to some reluctance to perform the procedure unless the glaucoma was severe, or the pressure was very high. As a result of those issues there has been a search during the last 40 years for something that had a lower complication rate and could be more easily deployed earlier in the disease process.
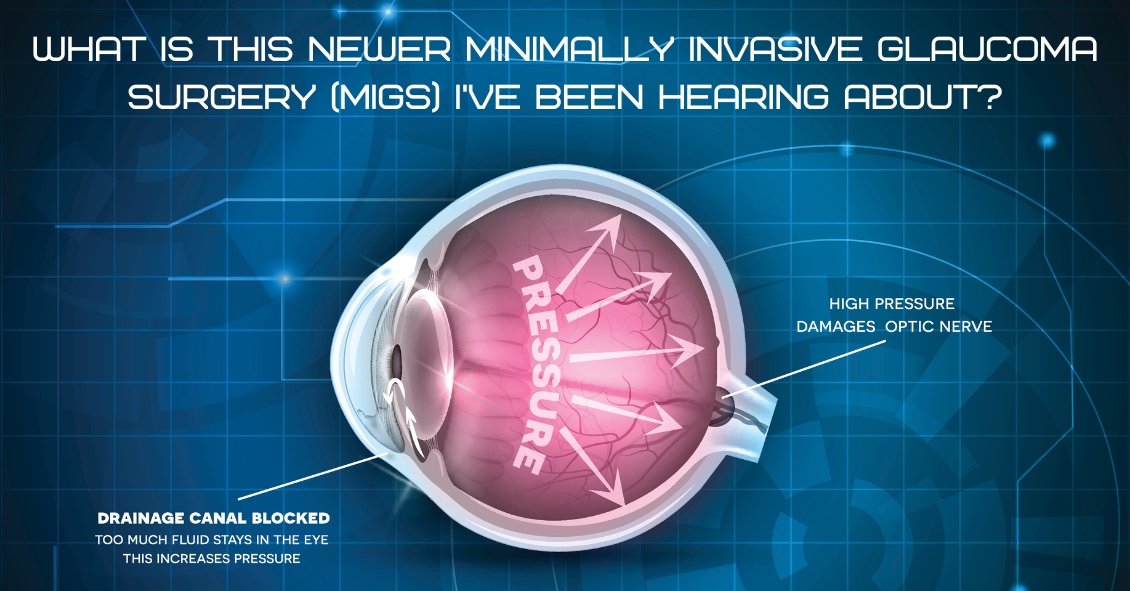
Enter Minimally Invasive Glaucoma Surgery, or MIGS. There are now several types of surgeries that fit in the MIGS category and many of them are used in conjunction with cataract surgery. They are utilized much earlier in the disease process and when combined with cataract surgery they can be used to not only help control the pressure over the long term but can often even reduce the burden of eye drops afterward.
The biggest advantage to MIGS over the trabeculectomy is that when used in conjunction with cataract surgery, MIGS can lower the eye pressure (although not as much as the trabeculectomy) but often with no higher rate of complications as there is with cataract surgery alone.
The lower complication rate is mainly because the MIGS procedures do not create a full-thickness hole in the wall of the eye. Most of them involve putting in some form of stent inside the eye. The stent lets the intraocular fluid get out of the eye more efficiently through its normal internal drain called the trabecular meshwork, rather than having to flow to the outside of the eye as with a trabeculectomy.
A stent is not the only way to lower the pressure along with cataract surgery. There is also a laser treatment you can do from the inside of the eye that slows the amount of fluid the eye makes, which also results in a lower pressure. It is called Endocyclophotocoagulation (ECP). Think of a partially clogged drain in a sink with constantly running water. If you don’t want the sink to overflow (or the pressure in the eye to get too high) you either try to unclog the drain (stent) or you turn down the faucet (ECP).
MIGS has been a great development over the last several years, enabling the surgeon to intervene at a much earlier stage of glaucoma and with a significantly lower complication rate than the more invasive trabeculectomy.
At this point I utilize one of the MIGS procedures in almost all patients who need their cataracts removed and are on one or more glaucoma medications. Even if the glaucoma is fairly well controlled at the time, the MIGS procedure gives us the opportunity to try and get a glaucoma patient off their eye drops, which is both a decreased burden of treatment and lets us keep the eye drops in reserve should the pressure start to increase again later in life.
If you have glaucoma and a cataract you should definitely discuss this with your doctor to see if a MIGS procedure along with your cataract surgery could be the right choice for you.
Article contributed by Dr. Brian Wnorowski, M.D.
If it's been a while since your last eye exam--or if you've never had one done--it's always nice to know what testing you might have done and what issues the eye doctor looks for. Here's the scoop on some common testing...
Visual Field
The visual field test is designed to check your peripheral vision, which isyour ability to see things where you are not directly looking.
When we test your vision on the basic eye chart, we are testing how well you see right in the center and it gives us no idea if you can see out away from the center. Your peripheral vision is very important because it gives you the ability to move around your environment without running into things.
There are several diseases that can severely impact your peripheral vision while leaving central vision unaffected. Some people can have perfectly normal 20/20 central visual acuity and have almost complete loss of their peripheral vision.
The main culprits that can have a big impact on your peripheral vision are glaucoma, some retinal diseases such as retinal detachments or retinitis pigmentosa, and some neurological problems like brain tumors, strokes, pseudotumor cerebri, and multiple sclerosis.
Most visual field tests are now done on an automated machine that flashes lights in your peripheral vision while you stare straight ahead. The lights continue to get dimmer until you can no longer detect that they are there. The machine is trying to find the dimmest light you can see at each point in your peripheral vision that it is testing for.
Many patients get anxious when they take this test because everyone wants to do well on it. That sometimes results in people not staring straight ahead but trying to look around to find the lights in an effort to do better.
That just makes the test come out worse. The machine also makes some noise as it changes location of the test light. Some people start pressing the buzzer whenever they hear a noise. They think there must be a light they missed but the machine, several times during the test, makes noise and then doesn’t put a light on to specifically see if you are trying to cheat by hitting the buzzer on the noise rather that seeing the light. Please don’t do those things - you are only cheating yourself and making it more difficult to figure out your problem.
Ocular Coherence Tomography (OCT)
The OCT really took hold in eye doctors' offices at the beginning of this century. It was the first time we were able to see anatomy and pathology inside the eye on a microscopic level without the use of any radiation.
It has been a great addition to our examination techniques and allowed us to see many causes of vision loss at a level of detail we never had before.
The two biggest uses for OCT in optical health are diagnosing diseases of the retina, particularly the area of central vision called the macula, and for diseases of the optic nerve, the most common of which is glaucoma.
For retinal disease it has been extremely helpful for macular problems such as macular degeneration (the leading cause of blindness in the U.S.), diabetic retinopathy, retinal vascular occlusions, and retinal swelling from inflammation.
The OCT allows us to see the individual cellular levels of the retina and helps in diagnosing the exact level where the pathology is occurring. If you look into the eye at the retina and see some bleeding in the macula it is difficult to judge where that blood exists. Is it superficial in the retina and coming from the retinal circulation or is it deep in and coming from the choroidal circulation under the retina?
The difference between those two locations can have a significant impact on what disease is causing the problem and what the proper treatment is. The OCT is also helpful in following the effect of treatment. If you are treating a bleeding or swelling problem in the retina, the OCT can track the degree of improvement with a level of detail that could never be matched by the human eye.
For glaucoma and other problems with the optic nerve, the OCT can precisely measure the thickness of the nerve tissue as it passes through the optic nerve. The hallmark of glaucoma is progressive loss of nerve fibers in the optic nerve. Being able to measure the nerve thickness down to the micron level assists in both diagnosing and watching for progression of any optic nerve disease.
Fundus Photography
A picture is worth 1,000 words...
Fundus photography is just that, a regular picture of the inside of your eye. The pictures highlight the appearance of the macula and the optic nerve and record it for prosperity.
As eye doctors we make notes in the medical record of what we see when we look in the eye. The wording of anything that looks abnormal with the retina or optic nerve does vary somewhat from doctor to doctor. One of things we record is something called the cup to disk ratio (C:D) of the optic nerve. We express that ratio as a percentage. Normal is about 30% or .3. The range of normal is very wide and some “normal” eyes have a .1 cup and others can have a .7.
In glaucoma those percentages get larger over time as the person loses nerve tissue. So, if you were born with a .3 cup but in your 60’s you were found to have a .5 cup that would be a strong indicator that you might have glaucoma. However, if you were born with a .5 cup and at 60 you still have a .5 cup then you don’t have glaucoma. When you look at someone at 60 with a .5 cup it’s hard to be sure if this is normal for that person or did they progress from a .3 cup to a .5 cup. If only I had a picture …
Pictures of the back of the eye really do tell the story better than words. I can describe what the C:D looks like to me but a different doctor may describe it differently. Doctors are usually fairly consistent in their estimate of the C:D when it is the same doctor watching that C:D over time. When a different doctor estimates the C:D that consistency is just not there. My .4 C:D may be my partner’s .5. But you can’t argue with the picture.
The same thing occurs with retinal bleeding. Rating the amount of bleeding as mild, moderate, or severe is somewhat helpful but there is a broad range of “mild” or “moderate”. When comparing two pictures taken at two different points of time it is much easier to decide if something is really getting better or worse.
We also use fundus photography to keep an eye on small tumors, called choroidal nevi, that can develop in the eye. These are increased areas of pigmentation under the retina in an area called the choroid. Most eye doctors explain these pigmented spots as “freckles in the eye.” Most choroidal nevi are small and fairly flat. They can, however, sometimes grow larger and rarely turn into a melanoma in the eye. Serial photographs are very helpful in watching the lesions for growth.
These three tests - visual field, OCT, and fundus photography - make up the core of our testing. There are many other tests that can be performed along with your eye exam but these three we described here probably make up about 80% of the tests you may encounter, depending on your eyes.
Article contributed by Dr. Brian Wnorowski, M.D.
This blog provides general information and discussion about eye health and related subjects. The words and other content provided in this blog, and in any linked materials, are not intended and should not be construed as medical advice. If the reader or any other person has a medical concern, he or she should consult with an appropriately licensed physician. The content of this blog cannot be reproduced or duplicated without the express written consent of Eye IQ.